
Limmer Education
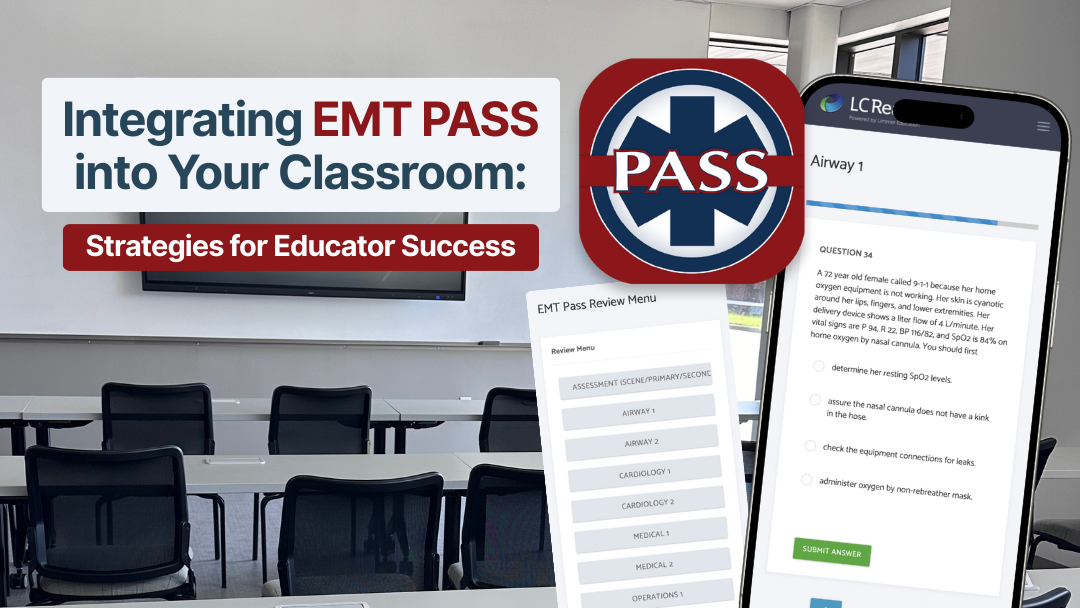
Practical strategies for integrating the app into your EMT curriculum.

by Chris Ebright
Our articles are read by an automated voice. We offer the option to listen to our articles as soon as they are published to enhance accessibility. Issues? Please let us know using the contact form.
Opioids, prescription and illicit, are currently the leading cause of drug overdose deaths. The current data from the Centers for Disease Control reports that 70,237 drug overdose deaths occurred in the United States in 2017. Opioids were involved in 47,600 of the cases (67.8% of all drug overdose deaths), and the sharpest increase in drug overdose fatalities was related to fentanyl and associated analogs (nearly 30,000 of the 47,600).
Update: The most recent CDC numbers show an even higher opioid death rate. Of the 107,000 drug overdose deaths in the U.S. in 2021, opioids were involved in roughly 75% of those cases.
The states with the highest rates of death (in order) were West Virginia, then Ohio, Pennsylvania, the District of Columbia, and Kentucky.
Opioid overdoses treated in emergency departments rose 30% from July 2016 through September 2017 in 52 areas within 45 states. Overdoses in the Midwest increased by 70%, and opioid overdoses in large cities increased by 54% in 16 states in that same time period.
Update: As of 2021, the states with the highest death rate (in order) were West Virginia, Tennessee, Louisiana, Kentucky and Delaware.
Needless to say, EMS personnel will likely encounter a patient suffering from an opioid overdose sometime during their career.
A 30-year-old female is dropped off at the front door of your ambulance station. The doorbell is rung, but when you approach the door, no one but her is present. The patient is unresponsive, limp, and cyanotic. Her airway appears to be clear of obstruction. She is breathing shallowly at four breaths/minute with auscultated rales in the bases of both lungs. Pulse oximetry reads 65% on room air. The patient’s other vital signs are heart rate, 106 beats/min. and irregular; blood pressure 92/64 mmHg; CO2, 70 mmHg; blood glucose 80 mg/dL; and temperature, 99.60. Further physical exam reveals pinpoint pupils and both her upper extremities appear to be covered with what look like needle tracks, multiple abscesses, and bruises in various stages of healing. Her skin turgor is poor with signs of malnutrition and dehydration. Two transdermal medication patches are found on the back of her right thigh.
Opioid toxicity should be suspected when CNS depression, respiratory depression, and pupillary constriction are present. The human body has three main opioid receptors, located in sensory nerves, mast cells, and in cells of the GI tract. Stimulation of these receptors generally results in euphoria, decreased perception of pain, and drowsiness. Mast cell effects (e.g., flushing, itching) are also common. GI effects include nausea, vomiting, and constipation. With most users, peak opioid effects are reached in ten minutes with the intravenous route, ten to fifteen minutes after nasal inhalation, and thirty to forty-five minutes with the intramuscular route.
When overstimulated, opioid receptors desensitize the brainstem to rises in carbon dioxide, which causes respiratory depression, loss of protective airway reflexes and respiratory arrest. Cardiac arrest from opioid overdoses is usually secondary to respiratory arrest. Death results primarily from hypoxia due to apnea.
Lesser common causes of morbidity and mortality from opioid toxicity are acute lung injury and pulmonary edema, status epilepticus, and cardiotoxicity. Many long-term users may also develop adverse effects due to the introduction of contaminants into their product. Cardiac, pulmonary, and hepatic damage may also be evident due to infections such as HIV, endocarditis or hepatitis (spread by needle-sharing and non-sterile injection techniques).
Serotonin syndrome occasionally occurs when certain opioids such as fentanyl, Demerol, codeine, or oxycodone are taken along with Selective Serotonin Reuptake Inhibitors (Paxil, Celexa, Prozac, Zoloft, etc.) or Monoamine Oxidase Inhibitors (Nardil, Marplan, Parnate, etc.). It typically presents with one or more of the following signs or symptoms: agitation, restlessness, confusion, tachycardia, hypertension, hyperreflexia, diaphoresis, seizure, muscle tremors, dilated pupils and a core temperature greater than 100°F.
The overriding goal of treating an opioid overdose is to restore respiratory drive and airway reflexes, prevent respiratory and cardiac arrest and avoid causing severe opioid withdrawal.
The first step is to evaluate the extent of the patient’s respiratory depression. Even if naloxone is clinically indicated, ventilatory support should always be provided immediately. Bag-valve-mask ventilation, including inserting oropharyngeal or nasopharyngeal airways, should be used to provide adequate oxygenation and ventilation until the patient can breathe adequately. Ventilatory support by itself may result in patient recovery as the accumulated carbon dioxide is expelled, and thus naloxone administration is not necessary.
Assess waveform capnography and pulse-oximetry to guide ventilation rate and adequacy. Upon re-establishment of a gag reflex, position the patient in a recovery position, and be ready to remove any basic airway adjuncts. Have suction readily available to prevent aspiration of any gastric contents.

Patients that present in a prolonged respiratory arrest (especially in patients where ventilation and naloxone administration fail to improve their condition) should have advanced airway management such as a supraglottic airway device or endotracheal tube insertion as a consideration, based on the EMS provider’s level of certification. Be ready to differentially diagnose for other conditions that may prolong the respiratory depression. Blood glucose determination should be routine for altered mental status and may be a useful finding in this situation.
Opioid toxicity may also cause a patient to become bradycardic and hypotensive. Thus, determination of a central or peripheral pulse can be difficult. If a pulse is not detected, start chest compressions and attach defibrillator pads or an AED. The 2015 American Heart Association guidelines recommend standard BLS and ACLS practices for cardiac arrest secondary to opioid overdose.
Waveform capnography and capnometry can also be useful in this instance. If a capnography waveform appears with ventilation, even if a pulse cannot be detected, the patient has a functioning heart. AHA recommends, in this case, that naloxone be administered.
Naloxone reverses overdoses by binding to opioid receptors, blocking stimulation and restoring the patient’s airway reflexes. The need for rapid access to naloxone in the pre-hospital setting has expanded its use to include both first responders and laypersons in the forms of an auto-injector for intramuscular administration and a commercial nasal spray. Consequently, this recently has struck up numerous moral and ethical debates on professional medical websites and social media. Regardless of popular opinion of administration, a retrospective study which analyzed data from northern New England revealed that basic life support practitioners are as effective as advanced life support practitioners in naloxone administration.

Before the administration of naloxone, application of restraints in a potentially violent patient is advisable, especially in close quarters or the back of an ambulance. Common routes of naloxone administration include intravenous, intramuscular, and intranasal. There is some debate as to which route of delivery is most effective, but overall, the medication itself is extremely safe. One of the significant drawbacks is if it is administered too quickly and/or in high dose concentrations. The common side effects of such include restoration of spontaneous breathing, but with associated extreme patient agitation, vomiting, and tachycardia. More severe, but rarer, reactions include signs of opioid withdrawal syndrome (OWS). Findings of naloxone-precipitated OWS include hypertensive emergency, seizure, pulmonary edema, ventricular tachycardia, ventricular fibrillation, and sudden death - primarily due to the sudden release of catecholamines.
Thus, the dosing of naloxone should be based on restoring adequate breathing while minimizing the risk of opioid withdrawal symptoms. This is best accomplished with dose titration and careful monitoring. Typically, naloxone is recommended to be administered via the intravenous route, as it reaches peak blood concentration within minutes. However, the time it takes to establish intravenous access, combined with a long-time IV opioid abuser patient with poor vasculature, may delay naloxone administration.
A method gaining more popularity is intranasal administration. It results in a more gradual emergence from the effects of opioids and allows EMS personnel to restore ventilations and airway reflexes without causing severe opioid withdrawal. Where this method becomes more initially ineffective than the intravenous route is when the patient has co-ingested other substances. Alcohol, benzodiazepines, fentanyl and/or one of its analogs, such as carfentanyl, usually require a higher dose of naloxone not typically delivered via the intranasal route.
Initially, most opioid users do not intentionally seek out fentanyl or carfentanyl. However, these synthetics, which are 50-10,000 times more potent than morphine, have created a distinct concern among public safety and EMS personnel.
Given the prevalence of synthetic opioids, law enforcement and EMS agencies have become increasingly concerned about potential exposures while responding to medical calls, crime scenes, or during drug raids.
However, here are the facts. Fentanyl needs moisture to penetrate the skin, and toxicity can’t occur from merely being in proximity to the drug.
Inhalation is an exposure route of concern. Aerosolized fentanyl puts it in contact with mucous membranes of the nose and/or mouth, which may supply enough moisture to allow it to penetrate the body and enter the bloodstream. Factually, at the highest airborne concentration potentially encountered, an unprotected individual requires nearly 200 minutes of exposure to reach a dose of 100 micrograms of fentanyl.
Incidental contact of fentanyl on dry, intact skin is also unlikely to cause opioid toxicity. For example: If both palm surfaces were covered with concentrated fentanyl patches, it would take approximately fourteen minutes to receive 100 micrograms of fentanyl.
Thus, accidental exposures that are typically seen in the pre-hospital setting aren’t likely to result in opioid toxicity of first responders and EMS personnel.
Standard nitrile medical gloves and duty uniforms provide adequate dermal protection. If suspected fentanyl powder is found on skin or clothing, the dry powder should be brushed away, and then the area should be cleaned with soap and water. Alcohol-based hand sanitizers should not be used for decontamination, as they do not wash opioids off the skin and may accelerate dermal drug absorption.
Respiratory protection isn’t required for routine operations. In the extremely unlikely event that it’s suspected that drug droplets or particles are suspended in the air, standard disposable N95 masks provide sufficient respiratory protection. OSHA-approved protection for eyes and face should be used during tasks where there exists a possibility of splash to the face.
Scene safety, as always, is paramount. As this was a drop-off and she is unresponsive, there is no telling what she may or may not have on her person, or in her pockets. Be wary of needles, syringes with blood, etc. Take proper precaution by wearing gloves at a minimum and have eye and respiratory protection available. Based on her presentation, insertion of a nasopharyngeal airway and ventilation via BVM is established with good compliance, but she does not regain consciousness. The pulse oximetry reading increases steadily, and the capnometry reading decreases with every ventilation. Attaining a SpO2 higher than 94% and a CO2 between 35-45 mmHg is ideal. Her blood pressure and pupils remain unchanged.
It is imperative to perform a good head-to-toe examination in this case, and ones similar, in which the patient is a poor historian. Doing so reveals the two medication patches. If these are prescribed fentanyl, the FDA mandates that they must have a name and strength in a visible color, but many patches will not have any identification. Even though research will say that these two patches may not deliver enough fentanyl to cause toxicity (especially in her case where she appears to be a long-time user), they can be safely removed with gloved hands and should be.
A peripheral IV line is easily established. The patient is administered a dose of naloxone that allows her to regain breathing at a rate of 12/minute. She is positioned in a left lateral recumbent position on the ambulance cot and transported to the local hospital. En route, a fluid challenge of normal saline is infused to increase her blood pressure, and she is supplied oxygen at 2 Lpm via nasal cannula, which maintains an adequate SpO2.
Scholl L, Seth P, Kariisa M, Wilson N, Baldwin G. Drug and Opioid-Involved Overdose Deaths – United States, 2013-2017. Morb Mortal Wkly Rep. ePub: 21 December 2018.
Centers for Disease Control and Prevention. Opioid Overdoses Treated in Emergency Departments. CDC Vital Signs. Available at https://www.cdc.gov/vitalsigns/pdf/2018-03-vitalsigns.pdf. March 2018.
Opioid Toxicity Clinical Presentation. December 13, 2018. Medscape. Available at https://emedicine.medscape.com/article/815784-clinical#b3. Accessed: June 5, 2019.
Opioid Toxicity and Withdrawal. March 2018. Merck Manual. Available at https://www.merckmanuals.com/professional/special-subjects/recreational-drugs-and-intoxicants/opioid-toxicity-and-withdrawal. Accessed June 5, 2019.
Opioid Toxicity Pathophysiology. December 13, 2018. Medscape. Available at https://emedicine.medscape.com/article/815784-overview#a5. Accessed: June 5, 2019.
National Institute on Drug Abuse. Overdose death rates [about 7 screens]. Rockville (MD): National Institute on Drug Abuse; 2018 August [cited 2018 Sep 26]. [Internet]. https://www.drugabuse.gov/related-topics/trends-statistics/overdose-death-rates
Lavonas EJ, Drennan IR, Gabrielli A, Heffner AC, Hoyte CO, Orkin AM, Sawyer KN, Donnino MW. Part 10: special circumstances of resuscitation: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Cardiovascular Care. Circulation. 2015;132(suppl 2):S501–S518.
Williams K, Lang E, Panchal AR, Gasper JJ, Taillac P, Gouda J, Lyng JW, Goodloe, JM, Hedges M. Evidence-Based Guidelines for EMS Administration of Naloxone. Prehospital Emergency Care. 17 Apr 2019. https://doi.org/10.1080/10903127.2019.1597955. [Taylor & Francis Online]
Sullivan B. (2016, Jan.8). 5 things EMS providers need to know about opioid overdose and respiratory compromise. Retrieved from: https://www.ems1.com/ems-products/Capnography/articles/47753048-5-things-EMS-providers-need-to-know-about-opioid-overdose-and-respiratory-compromise/
Gulec N, Lahey J, Suozzi J, Sholl M, MacLean C, Wolfson D. Basic and advanced EMS providers are equally effective in naloxone administration for opioid overdose in Northern New England. Prehosp Emerg Care. 2018;22(2):163–9. doi:10.1080/10903127.2017.1371262. [Taylor & Francis Online], [Web of Science ®], [Google Scholar]
Lameijer, H, Azizi N, Ligtenberg JJ, Ter Maaten JC. Ventricular tachycardia after naloxone administration: a drug related complication? Case report and literature review. Drug Saf Case Rep. 2014;1(1):2. doi:10.1007/s40800-014-0002-0.
Kienbaum P, Thürauf N, Michel MC, Scherbaum N, Gastpar M, Peters J. Profound increase in epinephrine concentration in plasma and cardiovascular stimulation after mu-opioid receptor blockade in opioid-addicted patients during barbiturate-induced anesthesia for acute detoxification. Anesthesiology. 1998;88(5):1154-1161.
Kim HK, Nelson LS. Reducing the harm of opioid overdose with the safe use of naloxone: a pharmacologic review. Expert Opin Drug Saf. 2015;14(7):1137–46. doi:10.1517/14740338.2015.1037274.[Taylor & Francis Online], [Web of Science ®], [Google Scholar]
Drug Enforcement Agency. DEA Warning to Police and Public: Fentanyl Exposure Kills. 2016. https://www.dea.gov/divisions/hq/2016/hq061016.shtml.
McDaniels A. Deputy, two EMS providers treated for overdose symptoms responding to call. The Baltimore Sun, Baltimore, MD. 2017. http://www.baltimoresun.com/health/bs-md-harford-opioid-exposure-20170523-story.html.
Greenslade B. 3 Winnipeg police officers possibly exposed to fentanyl, self-administer naloxone. Global News. 2017.
American College of Medical Toxicology. ACMT and AACT position statement: preventing occupational fentanyl and fentanyl analog exposure to emergency responders. Phoenix (AZ): American College of Medical Toxicology; 2017 Jul 12. https://www.acmt.net/cgi/page.cgi/_zine.html/The_ACMT_Connection/ACMT_Statement_on_Fentanyl_Exposure
Taxel S. (2019, May 7). Fentanyl Facts and Fiction: A Safety Guide for First Responders. Retrieved from: https://www.jems.com/articles/2019/05/fentanyl-facts-and-fiction-a-safety-guide-for-first-responders.html
Limmer Education

Dan Limmer, BS, NRP
Dan Limmer, BS, NRP