

Limmer Education
Build a study plan that fits your life, identify the gaps holding you back, and practice in a way that strengthens critical thinking.
by Limmer Education
Our articles are read by an automated voice. We offer the option to listen to our articles as soon as they are published to enhance accessibility. Issues? Please let us know using the contact form.
The comments from a recent free NREMT review session made us realize that some important items were still being taught wrong—and at alarming levels. This post will highlight some of these substantial falsehoods and misconceptions in EMS.
Before we do that, a bit of history may help clarify why some of these misconceptions exist.
In 1994 the US Department of Transportation released the EMT-B curriculum. This curriculum eliminated any pathophysiology from EMT education and took a technician-level approach. Many of today’s EMS educators learned during the EMT-B period from about 1994 – 2009. People teach what they learned.

Adding to the problem, EMS is relatively young as a profession and immature in its approach to change. Even the thought that there may be more than one way to do something or that there may be more than one correct answer challenges our “do exactly what our instructor says” mentality.
This leaves some substantial misinformation being taught to students. Here are a few of the sacred cows we found lingering around the EMS pasture.
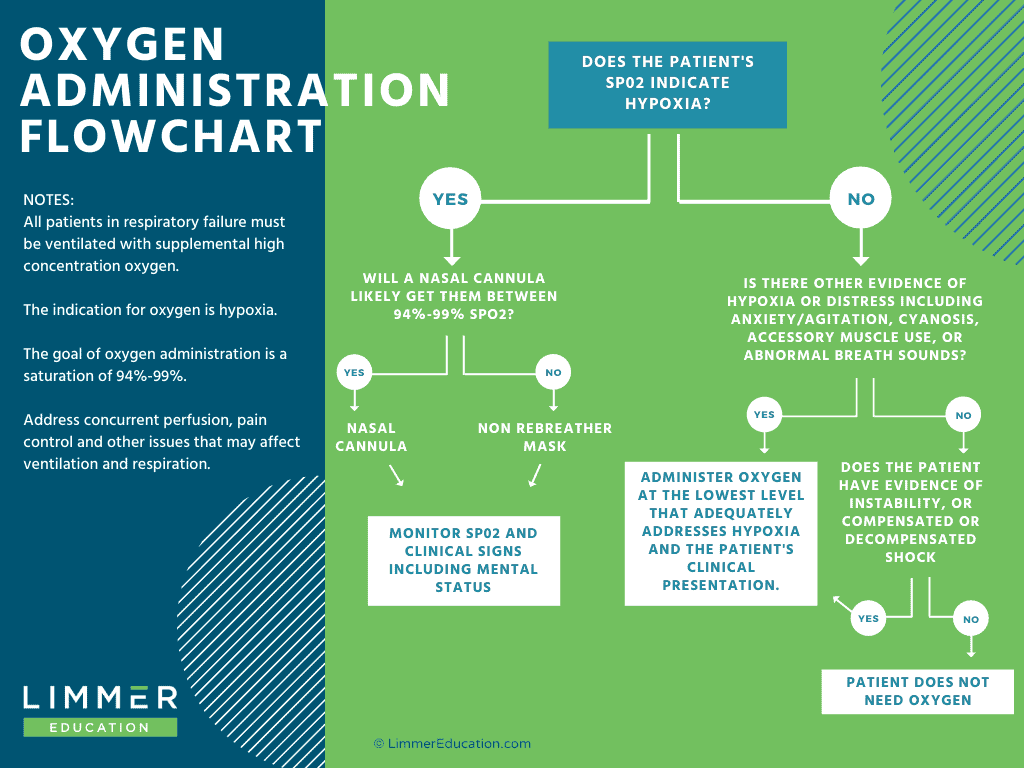
It seems that oxygen makes us feel better when we administer it. If only it had a benefit to non-hypoxic patients. We still seem to have a group of educators and providers who believe that we should pour on oxygen, but the literature and current guidelines don’t support it. (More on that here.)
Oxygen is a drug and should be provided based on indications…like hypoxia.
Our flowchart can help you choose the right oxygenation plan for your patient.
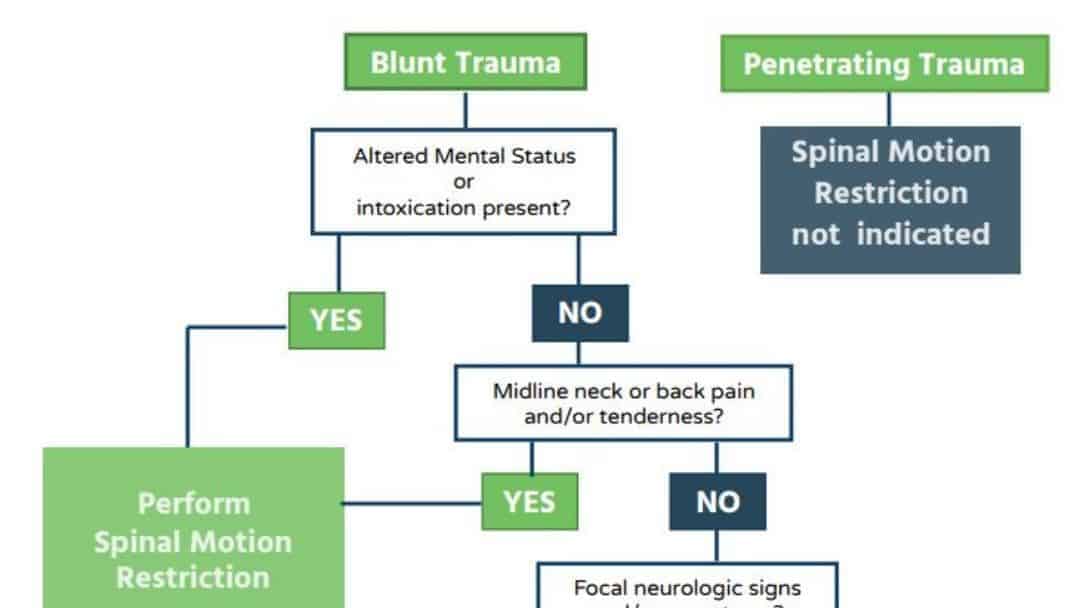
Position papers released in 2018 and supported by the National Registry say that we don’t immobilize patients on backboards any longer. Backboards cause pain—sometimes more than the injury itself. Securing the patient on the stretcher restricts motion and is much more comfortable. Our guide to assessing and performing spinal motion restriction can be found here.
Many students are still being taught to “stabilize” a flail segment with anything from bulky dressings to IV bags. These treatments are old. If a flail segment is big enough to limit ventilation, the only treatment should be to ventilate the patient. Restricting chest movement won’t increase ventilation—and may limit it!
Remember that the chest muscles will splint the flail segment naturally for a while. Paradoxical motion may not be visible initially. You will see that motion more prominently when the patient begins to tire. If the flail segment is large enough, you will need to ventilate.
Probably one of the most commonly taught but very wrong approaches is that we suction every newborn. Since 2010 the American Heart Association guidelines say only suction if there are signs of distress. Even in the presence of meconium, if there is a vigorous baby, we don’t suction.
Suctioning isn’t benign. It can cause hypoxia and bradycardia.
Should you apply a traction splint on an open femur fracture? A recent discussion we had on traction splinting showed differing opinions on this.
We believe you should apply the splint as long as it's an isolated, mid-shaft fracture. The benefits are: 1.) It gets the bone ends back in line, 2.) it relieves some of the pain and most importantly, 3.) it controls bleeding by leaving less space to bleed into. If you can irrigate the bone ends briefly with sterile saline, OK. But apply the splint. The bleeding control benefits outweigh the risk.
The number of times a traction splint is used is minimal. Again, application is limited to mid-shaft fractures with no other injuries–to the knee or hip, for example. Remember that many patients with these fractures have other concurrent injuries that make splinting the femur a lower priority (over treating for shock and prompt transport).
Limmer Education
Build a study plan that fits your life, identify the gaps holding you back, and practice in a way that strengthens critical thinking.

Limmer Education
Failing the NREMT doesn’t end your calling to become a paramedic. Diagnose why, adjust, and persist.

Limmer Education
Get the latest EMS guideline changes impacting trauma care, resuscitation, and education nationwide.
My orthopaedic surgeon said, “Of course use a traction splint on open fracture, they use Bucks Traction in the hospital. They do Open Reduction Internal Fixation and debride the heck out of it in the OR.” If it was on and bone went back in or open and sticking out, 2 muscles are still pushing & pulling and doing damage. HARE says no. Sager says yes. What dues your MD say?
Infusion of copious amounts of crystalloids into exsanguinating trauma patients.
I'm still seeing instructors who adamently advocate for the use of a bulky dressing for flail chest injuries. Not cool people...not cool!
Can you tell me with out a doubt that you know your patient is critical or not based solely on dispatch information
The question should be "will the use of red lights and siren change the outcome of the patient if dispatch is wrong? And additionally, "are seconds gained by use red light and siren going to change the outcome? If you answered NO, then red lights and siren are NOT indicated... Example: Law enforcement request EMS for a person that is not breathing, cold and stiff, and face is blue...No red lights and siren are needed...their dead...
Luckily recent studies have shown the "scared cow" of lights and siren on every call is not only unnecessary, but dangerous.