
Dan Limmer, BS, NRP
Don't psyche yourself out during the test. Here's what to do.

by Limmer Education
Our articles are read by an automated voice. We offer the option to listen to our articles as soon as they are published to enhance accessibility. Issues? Please let us know using the contact form.
In shock, there's a lot going on in the body – and if you know what you're looking for, you can detect the signs early, and without ever touching a blood pressure cuff.
Let’s look at the ways the body compensates for shock, how that affects vital signs, what happens when the body can no longer compensate for shock, and how emergency care providers can use all this knowledge to better help their patients.
In this article:
How does the body compensate for shock with heart rate? To answer this question, you need to understand the relationship between pulse rate (aka, heart rate) and cardiac output.
Remember this formula: heart rate x stroke volume = cardiac output. Let’s say someone’s pulse is 70 beats a minute. Each time you feel that pulse, 70 ccs (or mLs) of blood get pumped from the left ventricle. That means almost 5 liters of blood leave the heart every minute. (That’s the cardiac output.) That amount should provide the perfusion needed to stay alive and get oxygen to all the important parts of the body.
Heart Rate x Stroke Volume = Cardiac Output
How does cardiac output relate to shock? Well, if there’s volume loss in the cardiac output, the body has to start compensating for shock. So if the pulse stays at 70 beats a minute, but stroke volume (SV) drops to 50, you lose cardiac output.
Now say your patient has internal bleeding and the SV drops to 50 mLs. Every time the left ventricle squeezes, less blood is ejected. How does the body compensate? By raising the pulse. If the pulse increases to 100/minute (based on the equation above, now 100min x 50ml) the body is back to producing 5 liters of blood, allowing it to maintain perfusion.
That's how the body starts to compensate for shock. It increases the pulse rate to make up for the lower volume in each of those contractions of the left ventricle. If stroke volume goes down because of low volume (as in the case of bleeding in the belly or chest), then heart rate goes up to increase cardiac output.
But increased pulse isn’t the only way the body compensates for shock.
In response to shock, the body can also change the size of the blood vessels. By increasing vascular tone, the blood vessels get smaller. You can see increased vascular tone on the outside of the body, especially around the skin.
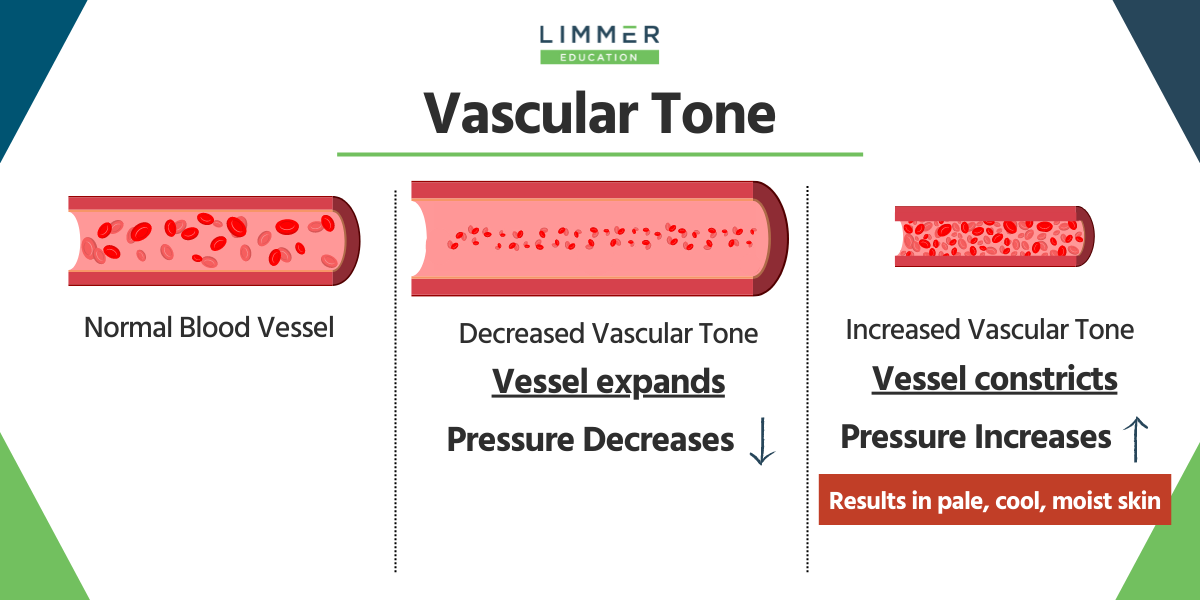
Vascular tone controls something called vascular resistance (or systemic vascular resistance). Basically what it comes down to is this: You have a blood vessel that’s a certain size, and because there’s fluid (blood) in that vessel, it has a set pressure.
If that vessel expands, the pressure goes down. And if that vessel constricts, the pressure goes up.
Constriction of the vessel is called an increase in vascular tone. Think of tone as being equal to squeeze. You’ve probably heard of the analogy where the heart is the pump and the pipes are the container. But did you know the body can alter the size of the “container” as a way to compensate for shock? As blood is lost, stroke volume drops and heart rate goes up – but the body still isn’t maintaining adequate perfusion. So, it increases vascular tone by making blood vessels smaller, thereby increasing pressure in the vessels.
However, this takes a toll – and we can see it on the outside of the body. If you see pale, cool, moist skin – think of shock. The skin appears this way because the vessels, all the small arteries and arterials around the skin, are constricted and shunting blood away from the skin. Blood is also going away from the gut because digesting food really isn’t a priority. That’s why there’s nausea and sometimes vomiting in shock!
So remember: Increase in vascular tone = smaller blood vessels and increased pressure. If a patient is experiencing this, you will be able to see it on their skin.
But pale, cool, moist skin isn’t the only way to detect shock during a primary assessment.
Remember that decompensated shock occurs when the body can’t maintain blood pressure anymore.
What other signs might you see in shock? Increased respirations. Because when there’s less blood, the body works to keep that blood as oxygenated as it can. Additionally, the body's tissues aren’t getting perfused, so there’s some anaerobic metabolism and acid buildup happening. Rapid respirations help blow off some of the CO2 that occurs.
Even though the body is trying to compensate and get blood to the brain and to the kidneys, the brain senses a lack of oxygen. Think of the brain like a furnace; it has to constantly burn fuel, but it can never get enough and there’s no fuel in reserve. If the brain doesn’t get oxygen and glucose, it starts to malfunction pretty quickly.
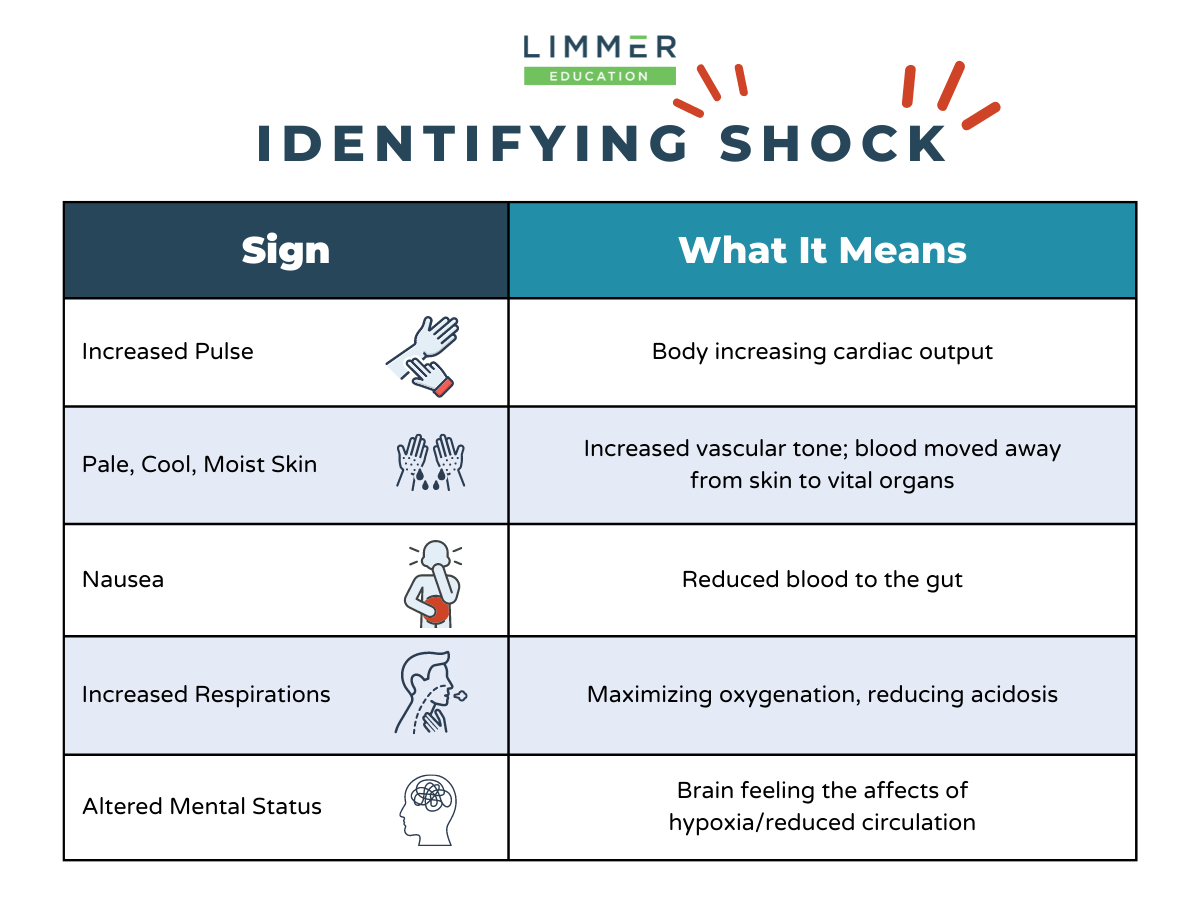
And that’s where altered mental status comes in. It’s the brain suffering from lack of oxygen and glucose. In the beginning, it might be anxiety or restlessness. But as shock progresses, it can turn into confusion or agitation – and ultimately lead to unresponsiveness.
increased pulse
increased respirations
cool, pale, moist skin
sometimes nausea
sometimes altered mental status
Now note that I haven’t spent a lot of time on blood pressure. Why is that? Because in your primary assessment as an EMT, you can find all of these things without using a blood pressure cuff. If you have an anxious patient with a rapid pulse, cool moist skin, and maybe breathing a little bit quickly, it shouldn’t be a surprise when you put that blood pressure cuff on that they are in shock.
Understanding the hows and whys is much more important than memorizing bullet points of individual conditions. Shock is shock. A patient that presents in a certain way should always make you think shock until proven otherwise.
Then at some point, they’ll no longer be able to compensate and the blood pressure will drop.
Pulse pressure is the difference between the systolic blood pressure (the top number) and the diastolic blood pressure (the bottom number). In a nutshell, pulse pressure is important because it can help us identify shock early in the patient encounter, sometimes before other symptoms occur.
Pulse pressure is the difference between the systolic blood pressure and the diastolic blood pressure.
Here’s an example: Let’s say the systolic is 120 and the diastolic 80.
The pulse pressure equation looks like this: Systolic-diastolic = pulse pressure
120-80 = 40.
The pulse pressure in a blood pressure of 120 over 80 is 40. Normal pulse pressure is about 25% of the systolic blood pressure. So with 120, I’d want at least 30. We’re at 40, so that’s great.
But let’s look at another example. A patient’s blood pressure is 102 over 88. You might initially look at 102/88 and think, “Well that isn’t too bad.” But when you calculate pulse pressure, you see there’s a problem. 102-88 = 14. The pulse pressure is 14 but it should be 25. That’s an early indicator of shock.
The systolic blood pressure ultimately represents cardiac output. It’s that squeeze in the ventricle. Diastolic represents vascular resistance. It’s what’s left after that big squeeze goes through. Remember, vascular resistance is the amount of tone or constriction in the blood vessels.
In shock, the body loses fluid whether through bleeding, dehydration, diarrhea, whatever it happens to be. Cardiac output drops, stroke volume drops, there’s only so much the body can do to compensate with increased heart rate. So then cardiac output drops, meaning the systolic number drops. But blood vessels in shock constrict. That means diastolic pressure is going to come up. So instead of 120 over 80, it’s 102 over 88. And that gives the patient a narrowed pulse pressure.
This is important in your patients as an early sign. When you see something like 102 over 88, think about what it means and why. Especially if you see other potential signs and symptoms of shock, like anxiety or skin color changes.
This matters for the National Registry too. The exam gives you a series of vital signs. Will you recognize that 102 over 88 as abnormal and potentially an indicator of shock? Because that might be the only indicator in the question that the patient is potentially unstable.
Pulse pressure has a very important role in identification of shock. It requires you to take a good, accurate blood pressure and pay attention to the readings.
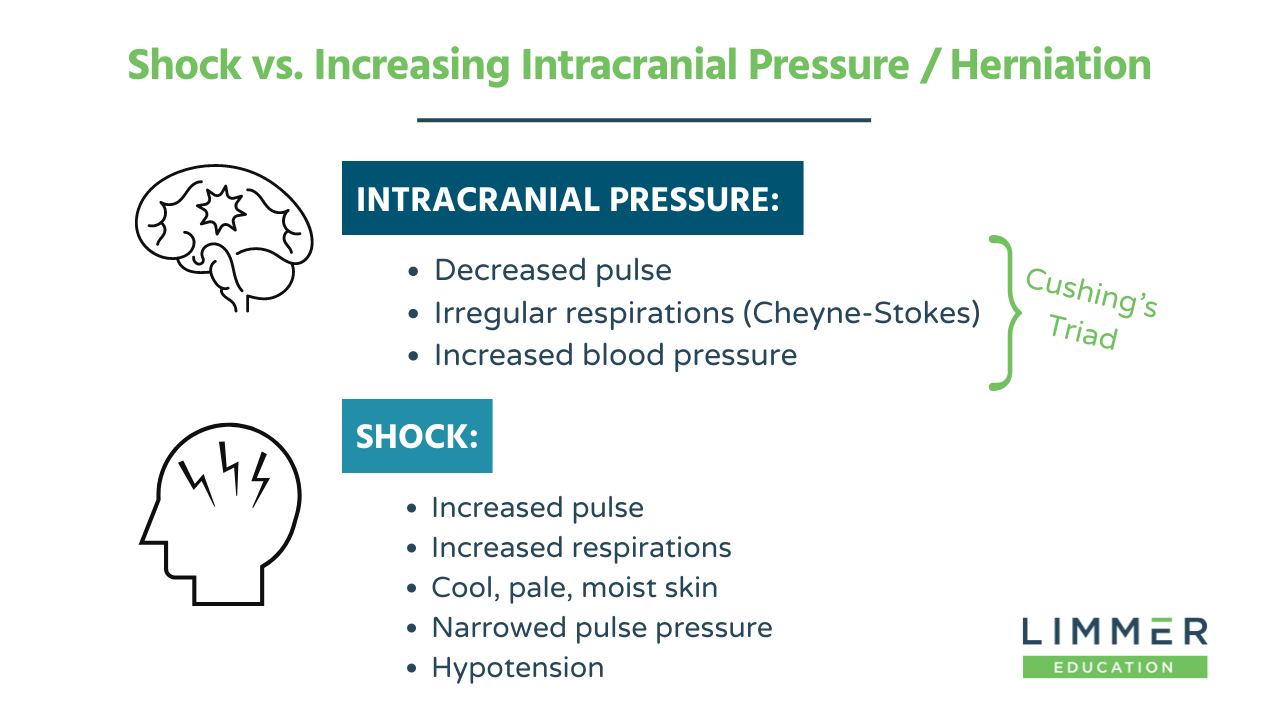
When it comes to rising intracranial pressure (or brain herniation), you need to know that the vital signs are pretty much the opposite of what you’d see in shock.
A patient was struck on the head and has a hematoma building in their head. As that blood gathers, it essentially squishes the brain down. It only takes about 50 ml of blood to start putting pressure on. The skull is a closed container so herniation pushes the brain down through the foramen, which is that large hole in the bottom of the skull where the spinal cord comes out. As the pressure increases, the brain fights to keep getting oxygen and glucose. The way it fights is by raising the blood pressure in the body. When this happens, in order for blood to pump out the aorta and up into the head, the blood pressure might get ridiculously high -- something like 150 over 90, 180 over 100, 220 over 120.
The blood pressure keeps rising because it's fighting to get blood to the brain where all that intracranial pressure is building. It’s the body’s way of saying, “I must feed the brain at all costs.”
However, not all parts of the body get the memo that feeding the brain is the priority.
Pressure receptors in the body react to the extremely high blood pressure by sending a message to the parasympathetic nervous system to slow down the heart rate. Because in order to lower blood pressure, the body has two choices: Reduce stroke volume or reduce heart rate. But in the case of brain herniation, reducing heart rate works against what the body’s doing using high blood pressure to keep oxygen and glucose going to the brain.
Now the body is basically fighting against itself. There’s extremely elevated blood pressure, and in response to that, there’s a low pulse.
Now let's talk about what happens to respiration during brain herniation. There’s a lot of pressure on the brainstem. The brainstem controls respiration. When there’s too much pressure on the brainstem, respiration malfunctions.
If you see Cushing’s Triad (irregular respirations + elevated blood pressure + decreased pulse), it’s a good indication of increasing intracranial pressure. This is especially true if there’s trauma, like a car crash scene or a head injury the patient sustained the day before.
The important thing here is that the signs seen in intracranial pressure are the opposite of those seen in shock.
Being able to identify rising intracranial pressure allows you to recognize the criticality of the situation and get them transported to a hospital.
Hopefully, this helps you understand why we see what we see in shock and recognize how trends in vital signs for both shock and intracranial pressure are enough for you to quickly determine that your patient is getting worse before your eyes.
Dan Limmer, BS, NRP

Limmer Education
Dan Limmer, BS, NRP
Quick question on Pulse pressure and assessing Shock.
Both examples of BP 120/80 and 102/88 show that different indicators of shock.
120 / 80 = PP of 40 and normal PP for these numbers should be 30, which it is NOT an indicator of shock.
102 / 88 = PP of 14 and normal PP for this BP should be 25 ........ which IS a sign of shock
My question is what is MORE of an indicator of Shock. ...... Pulse Pressure or Mean Arterial Pressure (MAP) MAP, as I understand it, is a more accurate measure of Perfusion and Shock , can be defined as Inadequate Perfusion. If that is the case, BOTH examples used show, essentially, the SAME MAP's. ( 93.55 and 93.33) I'd appreciate your thoughts on this. Thanks, Seamus