
Dr. Bill Young
EMS providers should understand the pathophysiology of anaphylaxis.

by Limmer Education
Our articles are read by an automated voice. We offer the option to listen to our articles as soon as they are published to enhance accessibility. Issues? Please let us know using the contact form.
In a previous post, it was established that simulation is more prominent in paramedic education than in EMT education. Educator experience and full-time status at advanced levels probably tend to favor simulation, while the manikins are also pre-programmed with an ALS focus.
Yet, it is our belief that the EMT classroom has much to gain from the use of simulation. In our first post regarding simulation, there is an example of how simulation could help students identify and respond to patients in respiratory failure—and to note how the simulation could also help prepare for the National Registry cognitive exam. Here are a few more ideas on how to integrate simulation into your EMT classes. Remember, not every simulation experience has to be a full start-to-finish scenario.
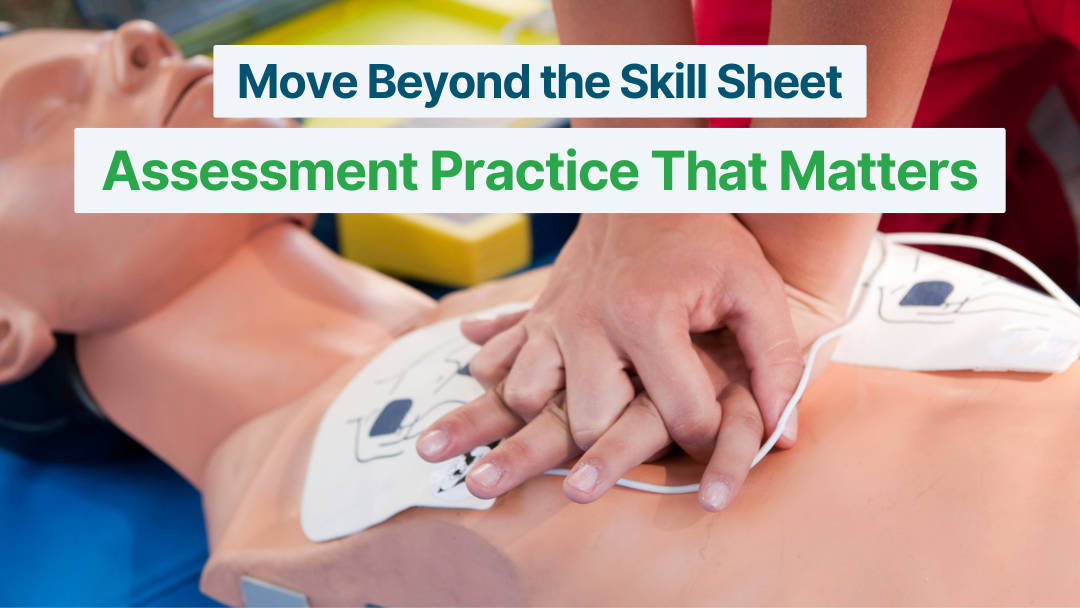
Have your students complete a primary assessment on the simulation manikin. Our students usually practice on each other, or a CPR manikin. Using simulation allows your students to truly assess respirations, hear snoring or gurgling sounds in the airway, and assess a variety of pulse and respiratory rates and patterns. Realistic injuries can demonstrate a need for bleeding control. Transform your student’s primary assessment from rote practice to decision-making quickly and easily.
With a manikin you can adjust:
The rate, rhythm, and strength of the pulse.
The rate and depth of ventilations.
The systolic and diastolic BP.
The pupils.
And more.
Vital sign practice on healthy classmates rarely shows any variation from normal.
One of the things that’s so impressive about the new ARES manikin is that it measures important CPR concepts, such as compression rate and depth, compression fraction, and whether the student is allowing full chest recoil. Compressing ARES’ chest is realistic in feel and demonstrates exactly how tiring fast and deep compressions are. Unlike CPR manikins, simulation manikins have the ability to produce carotid, radial, and femoral pulses of varied rates and strengths. One can also program the manikin to create realistic agonal breathing. Pump your CPR and AED training to the next level.
Hand the tablet that controls the manikin to a student or group of students and ask them to program a patient. Give them an asthma patient, a patient in shock, or one with increasing ICP. Facilitate the exercise as they discuss how the patient should present. You may also have one group create a patient and the other group has to assess the manikin and determine what’s wrong. This exercise is great for dynamic end-of-class practice sessions.
Some of these suggestions are relatively low-hanging fruit, but it is easy to forget how valuable simulation is—or to use simulation for only a fraction of its potential. I’d love to hear how you are using simulation in your BLS classes (EMT and EMR). What’s worked? What hasn’t?
You never know until you try.
Dr. Bill Young

Dan Limmer, BS, NRP

Mike Miller