

By Chris Ebright
You were taught from day one of taking vital signs to count respirations. However, I am here to say that your stellar EMT instructor let you down because she/he was wrong. The same incorrect terminology is also written in numerous textbooks, on run reports, and spoken everyday between medical professionals. So now you’re asking: Ok, smartypants, then what is the proper term? The appropriate term, my fellow professionals, is, you count – ventilations.
Aren’t these terms essentially the same? The easy answer is no. The harder question is: Well, why not? This installment of Back to the Basics discusses these physiological processes and how they differ. So please, read on.
Ventilation

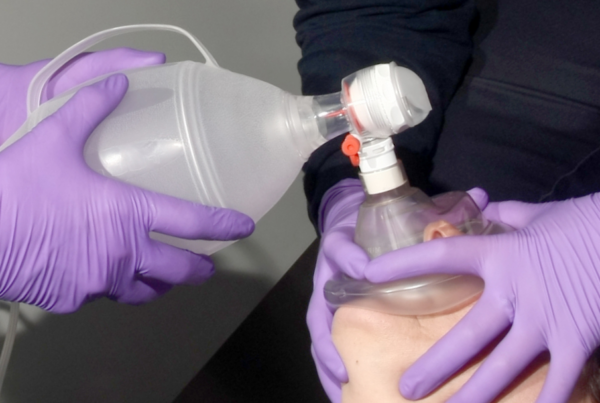
Simply put, ventilation is breathing – the physical movement of air between the outside environment and the lungs. Air travels through the mouth and nasal passages, then down the pharynx. Upon reaching the vocal cords, air flows into the trachea, transitioning from the upper airway into the lower airway. Here, it continues distally to the carina, then through the primary bronchi, various branches of bronchioles, and eventually arriving in the alveoli. This is inhalation. Air movement in a reverse pathway from alveoli to mouth and nose, is exhalation. Inhalation, followed by exhalation, equals one ventilation. This is what you observe (chest rise and fall) when determining the breathing rate.
A ventilation can only take place if the brainstem, cranial, and associated peripheral nerves, the diaphragm, intercostal musculature, and lungs are all functional. Combining the function of all these structures, the pulmonary ventilation mechanism establishes two gas pressure gradients. One, in which the pressure within the alveoli is lower than atmospheric pressure – this produces inhalation. The other, in which the pressure in the alveoli is higher than atmospheric pressure – this produces exhalation. These necessary changes in intrapulmonary pressure occur because of changes in lung volume.
So, how does the lung volume change? Quite simply, it is a combination of muscle contractions stimulated by the central nervous system, and the movement of a serous membrane within the thorax called the pleura. The pleura is made of two layers: a parietal layer that lines the inside of the thorax and a visceral layer that covers the lungs and adjoining structures (blood vessels, bronchi, and nerves). Between the visceral and parietal layers is a small, fluid-filled space, called the pleural cavity.
The initiation of ventilation begins with the brainstem, where impulses (action potentials) generate within the medulla oblongata, then travel distally within the spinal cord. The impulse traverses individually through cervical nerves three, four, and five until just above the clavicle. Here, the three cervical nerves merge into one large nerve called the phrenic nerve, which attaches distally to the diaphragm. Imagine these two nerves resembling a pair of suspenders on the anterior chest. The delivered impulse from the phrenic nerve initiates diaphragm contraction.
The intercostal muscles are a group of intrinsic chest wall muscles occupying the intercostal spaces. They are arranged separately in three distinct layers (external intercostal muscles, internal intercostal muscles, and innermost intercostal muscles). The intercostal nerves that stimulate these muscles originate from the spinal cord thoracic nerves 1-11.
Inhalation is initiated as the dome-shaped diaphragm is stimulated. As it contracts and flattens, the thorax expands inferiorly. The internal and innermost intercostal muscles relax, while the external intercostal muscles contract from stimulus by the thoracic nerves. This produces an upward and outward movement of the ribs (similar to the movement of a bucket handle), and the sternum (similar to when pulling upward on a handle of a water pump). The fluid in the pleural cavity acts like glue, adhering the thorax to the lungs. Hence, as the thorax expands vertically and laterally, the parietal layer drags the visceral layer along with it, causing the lungs to expand. Adequate expansion of the lungs results in a decreased pressure within the alveoli. Therefore, when the alveolar pressure drops below atmospheric pressure, air rushes into the lungs.
Remember, inhalation requires a stimulus initiated from the central nervous system. Think of it like turning on a light. The light stays unlit until you flip a switch (CNS), releasing electricity and stimulating the components of the light bulb. As long as the switch is on and there is an impulse, the light stays lit. However, if you turn off the switch, the stimulus ceases, and the light shuts down. Exhalation is akin to turning off the switch, so to speak.
Thoracic stretch receptors constantly monitor chest expansion. Once an acceptable limit of expansion develops, they send a message to the central nervous system to “turn off the switch.” All the nerves stimulating diaphragmatic and external intercostal muscle contraction temporarily stop conducting. Consequently, the diaphragm and the external intercostal muscles relax, decreasing the thoracic volume – like letting air out of a balloon. Assisting with this passive process, the internal and innermost intercostal muscles are stimulated. Their contraction pulls the ribcage and attached pleura further downward and inward, compressing the lungs and increasing the air pressure within the alveoli. Once the alveolar pressure exceeds the atmospheric pressure, air moves out of the lungs.
That is all there is to it – simple, right? Adults normally ventilate between 12 to 20 times per minute, thanks to the autonomic nervous system. We do not even have to think about it! Nonetheless, what becomes a problem (and why EMS gets a call) is when the nervous system, the thoracic musculature, or the lungs become diseased or disabled. Here is a partial list of pathologies that impair ventilation:
- Nervous system: brain stem injury/traumatic brain injury, cervical spinal injury, Myasthenia Gravis, ALS (Lou Gehrig’s disease), Guillain-Barré syndrome
- Thorax: blunt chest trauma, rib fracture/flail chest, diaphragmatic tear/hernia, penetrating chest trauma/pneumothorax, hemothorax, pleural effusion, compression of the chest
- Lungs: emphysema, chronic bronchitis, asthma, foreign body airway obstruction, cystic fibrosis, lung cancer/tumor
Respiration
Respiration is the movement of gas across a membrane. The gas exchange in the lungs is referred to as external respiration. The very thin membrane gas crosses is called the respiratory membrane, separating the air within the alveoli from the blood within pulmonary capillaries. Its structure consists of the alveolar wall, the capillary wall, and each’s respective basement membrane. A basement membrane is a thin, fibrous structure that separates the lining of an internal or external body surface from underlying connective tissue. Think of it like Christmas wrapping paper around a box.

Click for Larger Image
Recall that adequate ventilation enables air to reach the alveoli and establish a pressure gradient. The alveolar pressure of oxygen typically ranges from 80 to 100 mmHg, whereas the alveolar pressure of inspired carbon dioxide is very low (typically 40 mmHg). Oxygen-depleted blood, transported from the body’s cells and back to the right side of the heart, is pumped into the pulmonary trunk and through the pulmonary arteries. Eventually, the blood makes its way through the distal pulmonary capillaries surrounding the alveoli. Oxygen within the pulmonary bloodstream typically has a pressure of 40 mmHg, and carbon dioxide has a pressure of 45 mmHg. These differences in pressure allow for diffusion of oxygen from alveolar air, across the respiratory membrane and onto the hemoglobin of red blood cells. Carbon dioxide diffuses off hemoglobin, crosses the respiratory membrane, and enters the alveolar space.
The result of external respiration establishes a hemoglobin oxygen pressure in excess of 100 mmHg, and a decreased pressure of carbon dioxide of 40 mmHg. The exchange of oxygen and carbon dioxide continues across the respiratory membrane until the equilibrium of each gas is established. Oxygen-rich blood then flows from the lungs via the pulmonary veins back to the left side of the heart. Here, it is pumped out through the aorta to all body tissues.
Blood flows from the systemic circulation, down through arteries, arterioles, and eventually to the capillaries. Capillaries are only large enough to accommodate one red blood cell at a time, and blood flow at this level is very slow. This maximizes the time for the release of oxygen and reabsorption of carbon dioxide. Cells require high concentration oxygen to function correctly. Thus, another membrane exchange of gas must take place between individual body cells and the systemic capillaries.
This transaction occurs with gas already within the body, so it is termed internal respiration. Organelles within a cell take oxygen and combine it with glucose, fat, or protein, and make energy (ATP) through a series of complex chemical reactions. The resultant waste product is a high concentration of carbon dioxide. So, as arterial blood flows into capillaries, an awaiting cell has low oxygen pressure (40 mmHg, typically) and a high carbon dioxide pressure (45 mmHg).
Oxygen that is attached to hemoglobin maintains a pressure of around 100 mmHg, and carbon dioxide a pressure of 40 mmHg. A diffusion gradient is established once again, only this time in the opposite direction that occurred in the lungs. At the cellular level, the exchange of oxygen and carbon dioxide commences across the cellular/capillary membrane until an equilibrium of each gas is established. Blood flow continues through the venules, veins, vena cava, heart, and back into the lungs with a hemoglobin oxygen pressure of 40 mmHg and a carbon dioxide pressure of 45 mmHg. Rinse and repeat, every minute, of every day, for life.
Unfortunately, external and internal respiration can also be negatively influenced and inhibited by various disease processes. At the time of this article, the most notable respiratory pathology is caused by COVID-19, the coronavirus. View the YouTube video from the Cleveland Clinic’s Dr. Sanjay Mukhopadhyay (found in the reference listings) to get a first-hand view of what COVID-19 does to the alveolar-capillary membrane.
Additionally, here are some other common respiration pathologies:
- Pulmonary edema – left-sided heart failure
- Loss of surfactant – drowning/aspiration
- Pulmonary embolism – lack of capillary blood flow
- Internal/external hemorrhage – lack of blood volume returning to the heart
- Pulmonary contusion – blood collection in alveoli
- Atelectasis – various diseases that increase the size of the respiratory membrane
Hopefully, now you understand the difference between ventilation and respiration. Even though these are independent physiological processes, they are also mutually dependent to ensure the survival of the human body. So, the next time someone misuses one of these terms set them straight with a smile. Tell ‘em Chris told you.
Until next month…
Ventilation vs. Respiration Resources
- https://www.slideshare.net/cud2018/respiratory-1-pulmonary-ventilation-physiology
- Mukhopadhyay, Sanjay. (2020). https://www.youtube.com/watch?v=v2EHsG-C_Rg
- Panawala, Lakna. (2017). Difference Between Internal and External Respiration. Retrieved from: http://pediaa.com/difference-between-internal-and-external-respiration/
- Uchchhas, Nazib. (2017). Breathing and Respiration. Retrieved from: https://www.slideshare.net/uchchhas/breathing-respiration
About the Author
Chris Ebright is an EMS Education Specialist with ProMedica Air and Mobile in Toledo, Ohio, managing all aspects of internal continuing EMS education as well as for numerous EMS systems in northwest Ohio and southeast Michigan. He has been a Nationally Registered paramedic for 25 years, providing primary EMS response, land, and air critical care transportation. Chris has educated hundreds of first responders, EMT’s, paramedics, and nurses for 24 years with his trademark whiteboard artistry sessions, including natives from the Cayman Islands and Australia. Chris’ passion for education is also currently featured as a monthly article contributor, published on the Limmer Education website. He has been a featured presenter at numerous local, state and national EMS conferences over the past 13 years, and enjoys traveling annually throughout the United States meeting EMS professionals from all walks of life. Chris is a self-proclaimed sports, movie and rollercoaster junkie and holds Bachelor of Education degree from the University of Toledo in Toledo, Ohio. He can be contacted via email at c.ebrightnremtp@gmail.com or through his website www.christopherebright.com.
I have been stating this for years! I am glad someone took the time and wrote an article on the subject. You can not visually watch respirations!
[…] previous edition of Back to the Basics discussed the differences between ventilation and respiration. As long as those physiological processes are functional, pulmonary capillaries can suck up […]
[…] previous edition of Back to the Basics discussed the differences between ventilation and respiration. As long as those physiological processes are functional, pulmonary capillaries can suck up the […]